Physiotherapy Management of Diabetic Ulcers
Diabetic ulcers are a significant complication of diabetes, affecting approximately 15% of individuals with the condition. This blog provides an overview of diabetic ulcers, including their types, causes, risk factors, clinical features, assessment, and physiotherapy management.
Introduction
A diabetic ulcer is an open sore or wound commonly located on the bottom of the foot. These ulcers arise from factors such as poor circulation, high blood sugar levels, and nerve damage. The condition is further complicated by delayed healing due to restricted blood supply and infections. Understanding the types, assessment, and management of diabetic ulcers is crucial for effective treatment and prevention.
Types of Diabetic Ulcers
Neuropathic Ulcers
- Occur due to peripheral diabetic neuropathy without ischemia caused by peripheral artery disease.
Ischemic Ulcers
- Arise where there is peripheral artery disease without diabetic neuropathy involvement.
Neuro-ischemic Ulcers
- Result from a combination of peripheral neuropathy and ischemia.
Nature and Sites
- Diabetic ulcers are deep and spreading, commonly affecting the toes, soles of the feet, and occasionally, the legs, hands, fingers, and arms.
Diabetic Foot Ulcers
Diabetic foot ulcers are full-thickness wounds on the plantar surface of the foot. They are characterized by neuropathy, ischemia, and infection. High plantar pressures often cause these ulcers, especially at the second metatarsal head.
Etiology of Diabetic Ulcers
Diabetes affects nerves through two primary pathways:
- Free Radical Damage
- Rogue oxygen molecules damage cells, leading to inflammation.
- Reduced Vascular Supply
- Narrowing of arteries restricts blood flow, delaying wound healing and causing nerve damage.
High blood sugar levels and associated conditions (e.g., high cholesterol, hypertension) exacerbate these effects, leading to neuropathy, impaired sensation, muscle weakness, and abnormal foot structures.
Risk Factors for Diabetic Foot Ulcers
- Diabetes
- High cholesterol levels
- Coronary heart disease
- Hypertension
- Atherosclerosis
- Previous history of foot ulcers or amputations
- Poor glycemic control
- Smoking
Classification of Diabetic Foot Ulcers
The Meggitt-Wagner Classification outlines the severity of diabetic ulcers:
- Grade 0: No ulcer in a high-risk foot.
- Grade 1: Superficial ulcer without underlying tissue involvement.
- Grade 2: Deep ulcer penetrating to ligaments or muscle, no bone involvement.
- Grade 3: Deep ulcer with cellulitis, abscess, or osteomyelitis.
- Grade 4: Localized gangrene.
- Grade 5: Extensive gangrene involving the whole foot.
Clinical Features of Diabetic Ulcers
- Redness, swelling, or discoloration around the wound.
- Break in the skin, discharge, or itching.
- Dryness and pain.
- Thickened or callused skin around the ulcer.
- Fever and chills in advanced stages.
Assessment of Diabetic Ulcers
History Taking
- Ulcer onset, self-treatments, history of infection, and prior interventions.
- Medical history of diabetes, autoimmune, metabolic, or cardiac conditions.
- Surgical history, including previous amputations or debridement.
- Personal history, such as smoking or alcohol use.
Examination
- Skin Status: Visual inspection for peeling, maceration, and fissures.
- Neurological Status: Semmes-Weinstein monofilaments or 128 Hz tuning fork to assess sensation.
- Vascular Status: Checking pedal pulses, capillary refill time, and Doppler ultrasound findings.
- Ulcer Evaluation: Noting site, size, depth, discharge, and surrounding tissue condition.
Imaging
- X-rays for deep wounds and MRI for detecting osteomyelitis or abscesses.
Physiotherapy Management
Physical Therapy Modalities
- Thermotherapy
- Infrared lamps and ultrasound therapy improve blood flow and cell metabolism.
- Electrotherapy
- Electrical stimulation enhances wound repair.
- Shockwave Therapy
- Focuses sound waves to improve soft tissue healing.
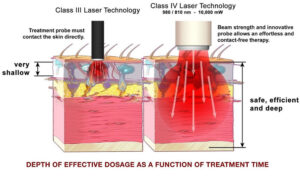
- Laser Treatment
- Effective for microcirculation and pain relief.
- Galvanic Current
- Direct electrical current for tissue repair.
Exercises
- Range of motion, stretching, Buerger-Allen, and proprioception exercises enhance blood flow and sensory input.
Shoe Modifications
- Special shoes with rocker bars, plastazote insoles, and proper cushioning distribute pressure evenly and reduce injury risks.
Nutrition Advice
- Adequate intake of iron, vitamins (A, B12, C), zinc, and proteins is essential for wound healing.
Prevention of Diabetic Ulcers
Primary Prevention
- Improved glycemic control and reduced cardiovascular risk factors.
- Routine foot examinations for early detection.
Secondary Prevention
- Quit smoking and avoid activities that may injure the feet.
- Daily foot inspections and proper hygiene.
- Use appropriate footwear and moisturizers (avoiding application between toes).
Conclusion
Diabetic ulcers are a complex yet preventable complication of diabetes. With appropriate physiotherapy modalities, shoe modifications, and preventive measures, patients can achieve improved outcomes and a better quality of life. Early intervention and comprehensive care play a vital role in minimizing the risks associated with diabetic ulcers.